PARAPARESIS-1
"PARAPARESIS"
I've been given this case data to solve in an attempt to understand and analyize the topic "PARAPARESIS" based on patient clinical data in order to develop competency in reading and comprehending clinical data related to Paraparesis and come up with a suitable diagnosis.
You can find the original case in the link below-
FOLLOWING IS THE PROBLEM LIST ACCORDING TO PATIENT'S PRIORITY:
MAIN COMPLAINTS:
- Weakness of both lower limbs
- Vomitings
- Gluteal abscess
- Scrotal abscess
EACH COMPLAINT IN DETAIL:
1. WEAKNESS OF BOTH LOWER LIMBS:
- ONSET:Sudden
- Since 5 days
- ASSOCIATED SYMPTOMS:Tingling and Numbness
- PAST HISTORY:had a fall when he got up for urination and was picked up by his father
- PROBABLE DIAGNOSIS:
- Peripheral Neuropathy
- INFECTIVE SPONDYLODISCITIS(spine infections-Most commonly-Tuberculosis)
- Gullian-Barre Syndrome/Multiple Sclerosis
- Sciatica
- Myasthenia Gravis
- Spinal lesion or tumor/Toxins
- INVETIGATIONS RECOMMENDED:
- X-Ray Spine
- CT SCAN and MRI
- Radionucleotide Imaging
- Blood culture,if due to some infection
- TREATMENT TAKEN:
- PHARMACOLOGICAL:
- Tab. Benadon-40mg/od =supplement of vitamin B6 given for proper functioning of the nerves
- Tab. Pregabalin-75mg/po/h/s =to treat pain due to nerve damage
- NON-PHARMACOLOGICAL:None
- TREATMENT RECOMMENDED:
- Antitubercular therapy(if TB is suspected)
- Treatment of the infection
- Rest
- Physiotherapy
- ONSET and DURATION: 5 days back
- PAST HISTORY:
- 3-4 episodes
- Non-projectile and Non-bilious
- CONTENT: Food Particles
- PROBABLE CAUSES:
- Infections
- Medication-induced vomiting
- Ingestion of toxins
- Emotional stress
- Tuberculoma
- Spinal tumors
- TREATMENT:treat the underlying cause/infection
- Since 5 months
- PROBABLE DIAGNOSIS:
- Injection site abscess
- TB of LUMBAR VERTEBRAE
- Psoas abscess
- Salmonella infection
- Amoebic gluteal abscess
- Crohns disease
- Carcinoma of colon
- TREATMENT GIVEN:
- NON-PHARMACOLOGICAL:
- Incision and drainage (operated 5 months back)
- Frequent position change recommended
- PHARMACOLOGICAL:
- Ointment Megaheal for local application
- Sitz Bath with BETADINE TID
- Since 20 days
- PROBABLE CAUSES:
- Bacterial Epididymitis secondary to tuberculous infection (most common)
- Testicular abscess that ruptures through tunica albuginea
- Drainage of appendicitis into scrotum through a patent processus vaginalis.
- TREATMENT:
- Incision and Drainage (done 10 days back)
- No similar complaints in past
- H/o multiple sexual partners
- Auto driver by profession( high risk behaviour)
- Not a known case of HTN/DM/ASTHMA/CAD
- The patient was conscious,coherent and cooperative
- Pallor,Icterus-absent
- No cyanosis,clubbing,lymphadenopathy,Edema
- VITALS-Normal
- All systems found to be normal
- CNS--Conscious with cranial nerves intact and speech-normal
- MOTOR SYSTEM:
- Normal Bulk of muscles
- Lower Limb muscles showed BILATERAL HYPOTONIA
- Lower Power of lower limb muscles
- SUPERFICIAL REFLEXES and DEEP TENDON REFLEXES:Present and Normal
- Absent PRIMITIVE REFLEXES
- Absent INVOLUNTARY MOVEMENTS
- SENSORY SYSTEM:Normal
- No Cerebellar or Meningeal Signs
- Elevated ESR (45mm/1st hr) ----->indicates INFECTION
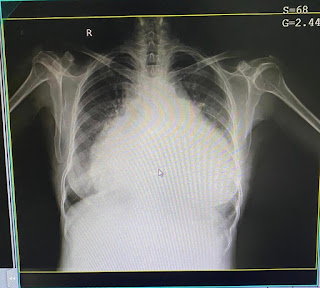
- X-Ray Shows:


--Multiple nodules in pulmonary apices suggest of pulmonary kochs and disseminated tuberculosis.
- MRI Shows:



Significant enhancement which represents meningeal enhancement or exudates and following lesions in MRI
DIAGNOSIS:
- Paraparesis with L4 , L5 INFECTIVE SPONDYLODISCITIS
- Left PSOAS ABSCESS
- Ring enhancing lesions in the cerebral hemispheres on MRI suggestive of PYOGENIC BRAIN ABSCESS---> maybe TUBERCULOMA
- with HEALING ULCER in RIGHT GLUTEAL REGION secondary to drained gluteal abscess
- with LEFT SIDED PYOCELE (operated 10 days back)
- ANATOMICAL LOCATION OF THE ROOT CAUSE:
- Pulmonary tuberculosis disseminating to the vertebral bodies and adjacent Intervertebral discs
- PHYSIOLOGICAL FUNCTIONAL DISABILITY:
- Weakness of lower limbs due to infection at various sites
- PATHOLOGY REFLECTING THE ROOT CAUSE:
- Mycobacterium tuberculosis, a slow-growing gram positive acid fast bacillus which becomes lodged in the bone via Batson’s venous plexus and lymphatic from primarily infected lung, lymph nodes, mediastinum and viscera, forming granulomatous inflammation and caseation necrosis.
- Primary or secondary involvement of the posterior appendicular and articular element along with paraspinal soft tissue can also be seen.
- Thoracolumbar region is the most commonly affected site while the cervical and sacrum regions are less commonly involved.
- Usually more than one vertebra is affected because of its segmental arterial distribution and subligamentous spread of the disease.
- " The bacilli reach the disc space causing disc destruction, spreads to adjacent vertebral bodies leading to vertebral collapse, anterior wedging, characteristic kyphotic angulation (Gibbus deformity), which may compress the spinal cord and nerve roots producing functional impairment."

Figure referred to the link --
www.ncbi.nlm.nih.gov › pmc › articles › PMC6179648IMPORTANT NOTE:
- The Infective Spondylodiscitis maybe due to Tuberculosis as various points turn the diagnosis towards Disseminated TB Infection.
- TUBERCULOUS SPONDYLODISCITIS is also known as POTT'S DISEASE.
CERTAIN POINTS:
Referring to this link --https://www.sciencedirect.com/science/article/pii/S2211568412001453.....the information goes as below:
- "Infectious spondylodiscitis is an infection of the intervertebral disc and the adjacent vertebral bodies due to the introduction of a pyogen, usually by the haematogenous route.
- Plain film radiography (which is usually normal in the early stages) shows blurring of the vertebral endplates and a loss of disc height that progresses quickly.
- MRI is the examination of choice, as it detects oedema within the trabecular bone very early, before the onset of destruction.
- Imaging can also be used to guide a needle aspiration to investigate the infective agent."
- Clinically, the infection is often sub-acute at onset, with inconsistent presentation of inflammatory signs on laboratory tests and concomitant visceral tuberculosis.
According to the source --
- "On imaging, there are three signs clinicians should be aware of:
- spinal cord compression is common
- centrosome geodes, often mirrored in another part of the intervertebral disc and often visible at multiple levels of the spine, sometimes combined with lesions of the posterior arch
- bi-lobed epidural abscesses that are often large, with distinct margins and that remain localised under the anterior longitudinal ligament. Due to these voluminous abscesses, carrying out frontal plane MRI views or coronal plane CT reconstructions is justified."
- Why the paraparesis due the tubercular infection of spine not associated with FEVER and other constitutional signs of TB???
- RECENT ADVANCES:
- The patient has been diagnosed with definite TB Infection which has disseminated to the spine and also caused the gluteal and scrotal abscess and also the pyogenic brain abscess(tuberculoma) and thus,has been started on Antitubercular therapy.
ACTIVE LEARNING AND CONVERSATIONAL DISCUSSION SUPPORT TO TREATING TEAM OF THIS CASE :
[5/22, 23:51] MBBS 2016 UG 3: Sir was the lumbar puncture done in the patient to diagnose TB?
[5/22, 23:53] Post residency PG1: Check out the conversations with your colleagues posted here
https://medicinedepartment.blogspot.com/2020/05/frequently-asked-questions-around-case.html?m=1 and you will get the answer
[5/22, 23:58]MBBS 2016 UG 3: Ok sir...thank you
ACTIVE LEARNING AND CONVERSATIONAL DISCUSSION SUPPORT TO TREATING TEAM OF THIS CASE :
[5/22, 23:51] MBBS 2016 UG 3: Sir was the lumbar puncture done in the patient to diagnose TB?
[5/22, 23:53] Post residency PG1: Check out the conversations with your colleagues posted here
https://medicinedepartment.blogspot.com/2020/05/frequently-asked-questions-around-case.html?m=1 and you will get the answer
[5/22, 23:58]MBBS 2016 UG 3: Ok sir...thank you

[5/22, 23:51] MBBS 2016 UG 3: Sir was the lumbar puncture done in the patient to diagnose TB?
ReplyDelete[5/22, 23:53] caregiver7careseeker: Check out the conversations with your colleagues posted here
https://medicinedepartment.blogspot.com/2020/05/frequently-asked-questions-around-case.html?m=1 and you will get the answer
[5/22, 23:58] MBBS 2016 UG 3: Ok sir...thank you