42 YEAR OLD FEMALE WITH MULTIPLE HEALTH EVENTS
THIS IS ALL ABOUT MY THOUGHTS AND SUBSEQUENT REVIEW REGRADING THIS CASE OF
"42 YEAR OLD FEMALE WITH MULTIPLE HEALTH EVENTS"
I have been given this case to solve in an attempt to understand the patient clincal data analysis in order to develop my competency in reading and comprehending clinical data
You can find the original case in the link below-
Following is my analysis on the patient's problem:
MAIN COMPLAINTS:
- Migraine with Aura
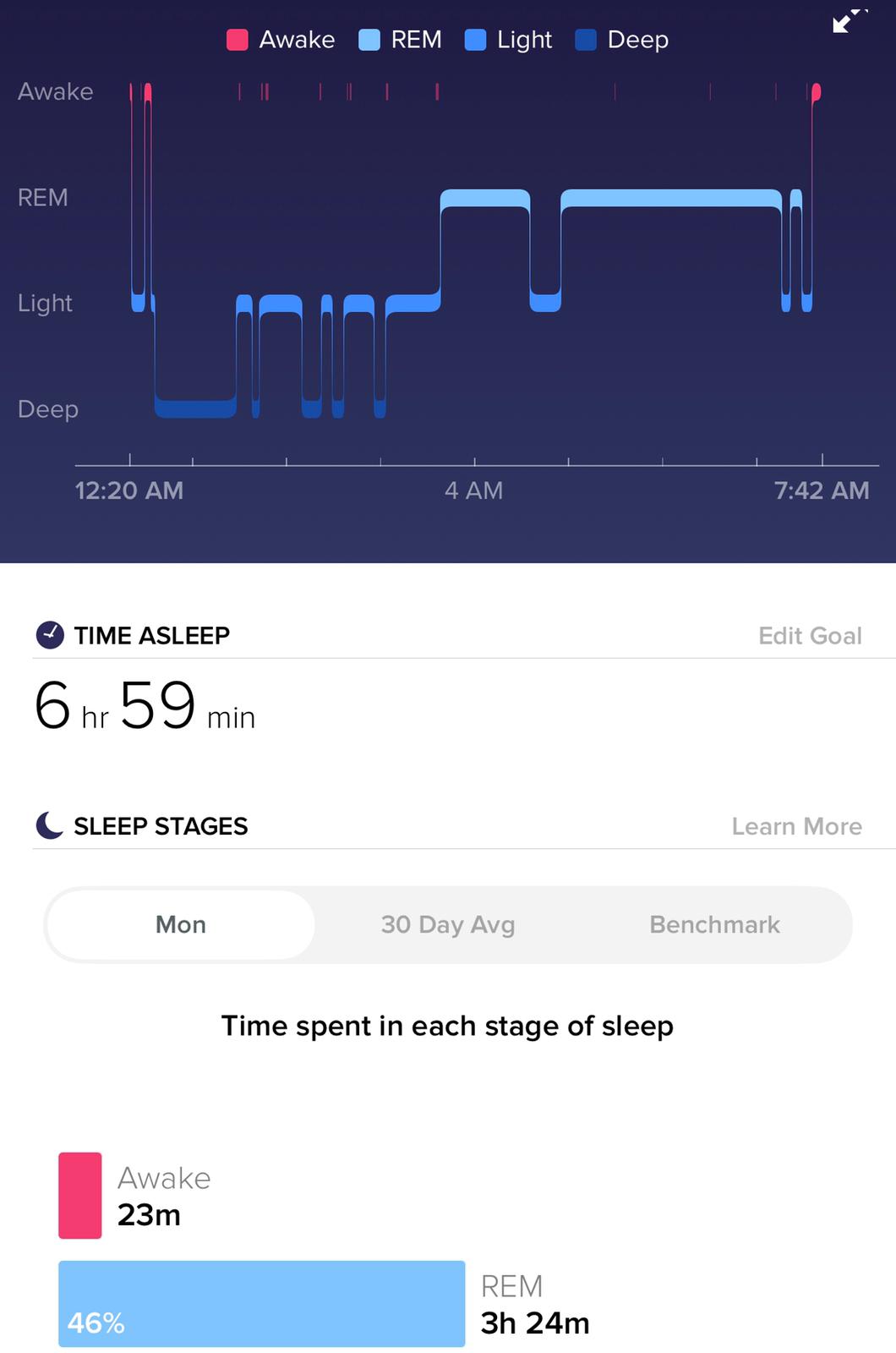
- Sleep Disturbances
- Edema mainly confined to face and abdomen
- Increased Pain Tolerance
- Fatigue
EACH COMPLAINT IN DETAIL:
- MIGRAINE :
- ONSET: Sudden
- DURATION: Since 2 years of age
- More towards the left side
- Gradually progressive
- ASSOCIATED SYMPTOMS:
- Numbness of left hand and left face felt like someone was pouring ice water over the cheek and also feeling of falling and spinning at night.
- Preceded by AURA associated with transient loss of vision
- Aura starts as a flicker and then eventually becomes a crescent that covers the entire centre of vision
- PAST HISTORY: It was also associated with stuttering and memory loss as well as loss of function of left side and an episode of CSF rhinnorhoea from left nostril.
- RELIEVING FACTOR : Medication (TRIPTANS )
- PROBABLE DIAGNOSIS:
- Hemiplegic Migraine
- Infections like meningitis, encephalitis (but she doesn't have a fever, rash).
- Brain tumours
- Seizures with post-ictal paralysis
- Mitochondrial Encephalopathy Lactic Acidosis and Stroke like episodes
2. SLEEP DISTURBANCES:
- ONSET: Since birth
- DURATION OF SLEEP: 2-4 hrs and no REM sleep
- POSSIBLE CAUSES:
- G6PD Deficiency impaired the glycolysis so glycine is not formed well . Glycine is also an inhibitory neurotransmitter.
- AMPD1 Deficiency can cause sleep disturbances because Adenosine is an inhibitory neurotransmitter so it should help in sleep.
- MEDICATIONS TAKEN: L-Serine , Cimetidine
3.EDEMA CONFINED TO FACE AMD ABDOMEN:
- ONSET: since 1 year of age
- DURATION: approximately 40 years
- SITE: Face , Abdomen
- AGGRAVATING FACTORS: Emotional Stress , Eating wrong food such as Fava beans , Exercise , Smoke
- RELIEVING FACTORS: Rest
- POSSIBLE CAUSES:
- Hemolytic anaemia could have led to right heart failure thus leading to pulmonary hypertension causing shortness of breath
- emotional stress and eating fava beans because she has G6PD Deficiency.
- This anaemia could be responsible for kidney infections as G6PD is required for producing NADPH which in turn is needed by the kidneys for their functioning. In G6PD deficiency, she could have had low NAPDH levels and thus kidney infections.
- TREATMENT:
- Avoid stress
- Do not consume fava beans, sulpha drugs, antimalarials
- Excess salt consumption
4. INCREASED PAIN TOLERANCE:
- Onset - since 4 years of age, still present
- ASSOCIATED COMPLAINS:
- History of multiple falls
- Fracture of ankle
- PROBABLE DIAGNOSIS:
- Osteoarthritis could be responsible for multiple fractures.
- CIPA (Congenital Intolerance to Pain With Anhydrosis )
5. FATIQUE:
- POSSIBLE CAUSES:
- AMPD1 deficiency - lack of ATP hence the person gets easily tired.
- Past history shows parents to be chain smokers which increases the oxidative stress.
- Oxidative stress from excess of free radicals because of G6PD deficiency
- TREATMENT: Ribose - provides ATP.
OTHER PROBLEMS:
- PCOS has led to:
- Dysmenorrhoea
- Hair Loss
- Ectopic Pregnancy
- Potential sensory disorder
- Severe Mood disorder
- Rashes on face-could be due to SLE
- Anxiety, depression, ADHD, Autism spectrum??
PAST HISTORY IN BRIEF(chronologically):
- At Birth , she had Severe Jaundice
- Tongue tie and upper lip tie
- Large upper tori
- Sleep disturbances(less than 3-4 hrs in a day)
- Edema of face/head and abdomen
- Vomitings, usually watery with salty broth
- Started speaking at 1 1/2 and writing in a language at 2 1/2 itself
- Excessive hair growth on face/neck/toes and legs at 3 years
- Didn't eat properly , i.e., anorexia maybe
- At 4yrs,Chronic UTI, Kidney infections, strep throat, lung infections, multiple sprained ankles and knees
- Severe reaction to Sulfa drugs
- Severe headache(since 2) -Worsens with menses and while on birth control=>MIGRAINE WITH AURA at age 32
- Potential sensory disorder
- Increased pain tolerance
- Severe mood disorder, on trying to calm down it usually precedes a swelling event or migraine
- At 12 , had Cervical degeneration and scoliosis
- At teenage, had anemia
- At 15,attempted suicide as headache worsened and she was bed forced
- Gained enough weight and was about 95lbs at 5'4" and ballooned up and fasted then to lose weight
- At 21,Ectopic pregnancy-she woke up during surgery
- At 22,had chronic abdominal pain and multiple ovarian cysts, diagnosed for PCOS on CT
- At 23,had Severe Kidney Infection and Pneumonia-at this event of hospitalization: Type aB melanoma and 4 precancerous tissues were removed
- At 30 , broke leg while dancing
- At 32, severe reaction to antimalarials-diarrhoea, vomiting, swelling, brain felt like slug. She also got swine flu and pneumonia-was vaccinated for pneumonia then
- At 34 , migraine with aura increased and was associated with transient loss of vision, stuttering, memory loss, left side of face and hand got affected. On lab investigations, poor liver function and mild hemolysis and high post meal cortisol were revealed.
- Anemia was diagnosed as haemolytic----genetic testing showed G6PD AND AMPD1 DEFICIENCY
- At 35, she had failed LASIK surgery and diagnosed of ADHD/Autism spectrum
CURRENT PROBLEMS:
- Frequent falls to left. Left foot started giving out as well as left hand. One fall downstairs broke sprained and broke left ankle
FRACTURE OF ANKLE

- Cravings for large amounts of salt and fats
- Swelling and hair loss
- Fatigue
- Left jaw pain upto face
- Struggle to breath --may be due pulmonary hypertension associated with right heart failure in anemia
- Intolerance to most foods and smoke
- Decreased sweating ( sweats only on emotional stress ,exercise,eating wrong thing, smoke )
- Decreased urination-Dark and yellow colored urinen after stress or exercise--this may be due to hemolysis due to G6PD deficiency.
- Decreased sleep ( nearly no REM ) --due to glycine crisis in AMPD1 and G6PD deficiencies.
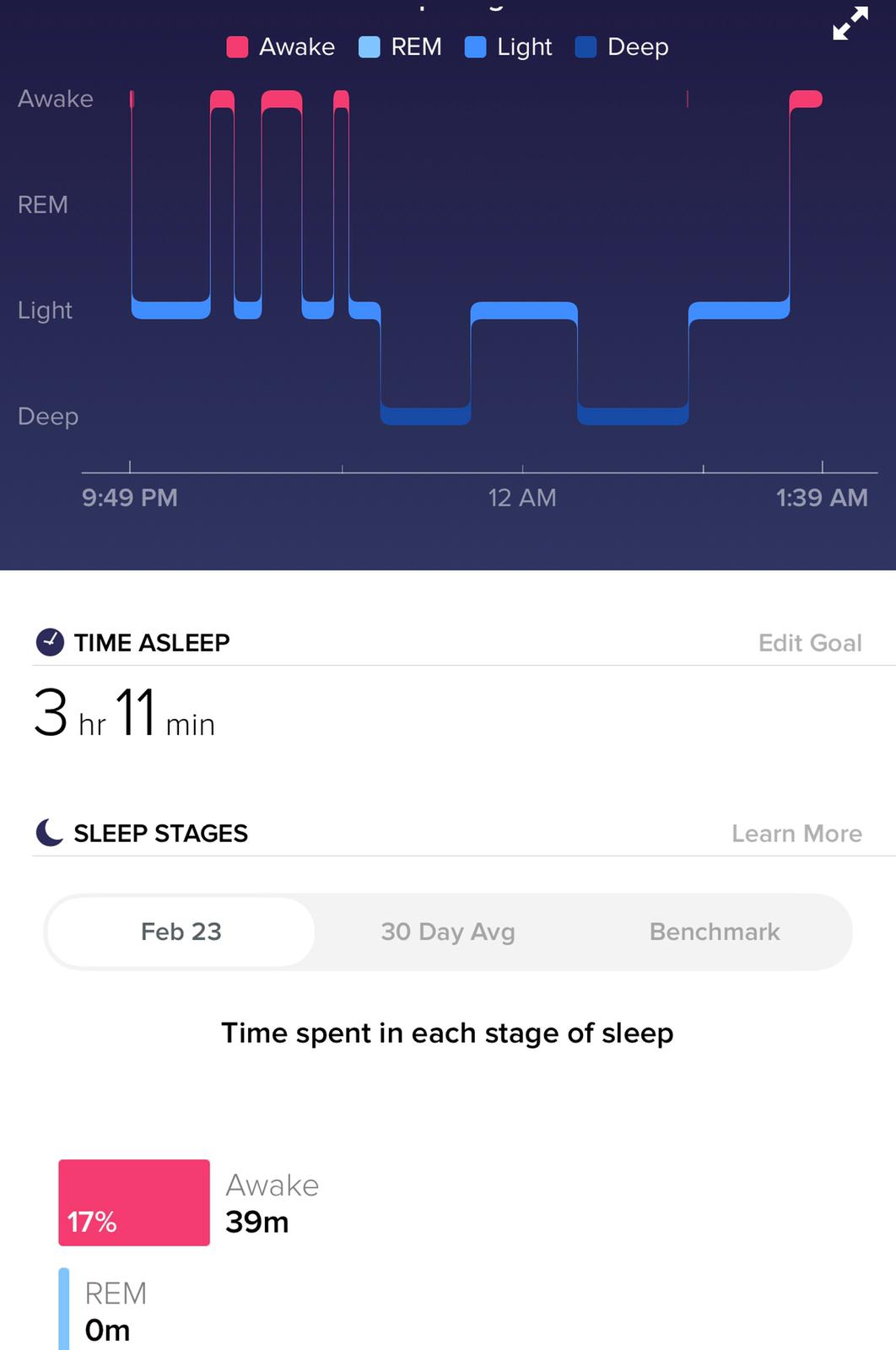
Sleep is decreased(nearly no REM)

Edema changes within weeks
CURRENT MEDICATIONS:
- L-Serine 20 mg at night to improve sleep
ON 1st DAY OF L-SERINE
- Ribose 2 gm every hour with water
- Cimetidine 400 mg to reduce swelling and in reducing androgens
- NAC 600 mg to increase glutathione antioxidants
- Iron folate 500% of rda
FOOD AND STRESS HAVE AN IMPACT ON HER EDEMA
CURRENT DIET:
- An apple once a day since many years.
- Now a days, 5% carbohydrates in diet, 95% other.
- Have tried many type of diets.
- Had been sick when followed dietician a year back
- Real unprocessed food
- Olive oil - 1/2 cup daily approx.
FAMILY HISTORY:
- Mother was diagnosed for fibromyalgia.
- Father had heart attack in 40s.
- Grand father had early death.
GENETIC WORKUP showed:
- Seattle type G6PD deficiency
- AMPD1 - AMPD1 deficiency heterozygous
- WNK1 mutation
- MTHFR - homozygous for C677T of MTHFR = 10-20% efficiency in processing folic acid = high homocysteine, low B12 and folate levels
- HLA-DRA - 3x higher risk for developing a peanut allergy In populations of European ancestry
- VWF - association with Von Willebrand disease type 1
- DIO2 - 1.3-1.79x risk of osteoarthritis, 3.75x bipolar, etc.
- CHRNA5 - higher risk for nicotine dependence, lower risk for cocaine dependence
- ANKK1 - Tardive Diskinesia risk, higher ADHD risk. More Alcohol Dependence. Lower risk of Postoperative Nausea. Increased obesity.
- TG - 1.3x to 11.5x Increased risk of autoimmune thyroid disease
- LOXL1 LOXL1-AS1 - common but 10x higher glaucoma risk in most (but not all) populations
- PNPLA3 - increased liver fat, odds of alcoholic liver disease
- BACE1 - 2x increased ALZ risk in ApoE4 carriers
- BSN - 1.1x risk Crohn's Disease
CONCLUSION FROM GENETIC WORKUP:
Increased risk for Alzheimer's, ADHD, Autoimmune thyroid & other autoimmune disorders, lung cancer, cluster headache, Obesity, raised ICP, Diabetes, RA, Bipolar disorders, Lung cancer and issue
SOME OF THE CLINICAL PICTURES PERTAINING TO THE PATIENT'S CONDITION:

Infant showed frontal bossing(raised ICT?)

 Rashes on Face
Rashes on Face - Usually 2-4 times a year. Past 6 months have not had one.
- Usually come with other issues and at that time WARTS and EBV have reactivated.
- The evidence of EBV being reactivated was that the labs were positive for EBV ONLY when she was sick

BLOOD BRUISE FROM BROKEN LEG remained unnoticed for long time as she had INCREASED TOLERANCE TO PAIN
POINTS OF CONCERN:
- Hemolytic anemia can also occur after eating fava beans or inhaling pollen from fava plants (a reaction called favism).
- Glucose-6-phosphate dehydrogenase deficiency is also a significant cause of mild to severe jaundice in newborns.
- Chemical reactions involving glucose-6-phosphate dehydrogenase produce compounds that prevent reactive oxygen species from building up to toxic levels within red blood cells.
- If mutations in the G6PD gene reduce the amount of glucose-6-phosphate dehydrogenase or alter its structure, this enzyme can no longer play its protective role. As a result, reactive oxygen species can accumulate and damage red blood cells. Factors such as infections, certain drugs, or ingesting fava beans can increase the levels of reactive oxygen species, causing red blood cells to be destroyed faster than the body can replace them.
- A reduction in the number of red blood cells causes the signs and symptoms of hemolytic anemia.
- Signs of glucose-6-phosphate dehydrogenase deficiency (G6PD deficiency) can begin any time from infancy to adulthood and vary in severity.
- Signs of G6PD deficiency include:
- Paleness
- Yellow skin tone (Jaundice)
- Dark urine
- Tiredness
- Shortness of breath
- Rapid heart rate
- Many of these signs may occur when your baby eats foods, like fava beans, which contain chemicals that cause the red blood cells to break down. They can also be triggered by certain drugs, illnesses, and infections.
- Adenosine monophosphate deaminase 1(AMPD1) deficiency, also known as myoadenylate deaminase (MADA) deficiency, is a disorder of purine metabolism that leads to a deficiency in the production of ATP.
- AMPD1 deficiency patients have generalized exertional muscle pain, cramps and fatigue. Other presenting features include post-exertional myoglobinuria and rhabdomyolysis.
FINAL TREATMENT OPTIONS:
- Symptomatic treatment has to be done as there is no cure.
- Avoid oxidants
- For hemolytic anemia: blood transfusion based on severity of anemia.
- Ribose diet-to reduce weakness
- L-serine for sleep disturbances
- Cimetidine for swelling
- cut down oxidative stress
- Antioxidants
- NAC
- Iron folate supplements
- Salt intake
RECENT UPDATE:
The patient has been diagnosed of BEHCET'S DISEASE which may be the reason for her rashes and mouth ulcers.
CERTAIN THINGS THAT REMAINED UNEXPLAINED:
-Failure of LASIK Surgery??
FUTHER INVESTIGATION SUGGESTED:
Advanced Diagnostic modality like Whole genome sequencing
REFERENCES
- https://ghr.nlm.nih.gov/condition/glucose-6-phosphate-dehydrogenase-deficiency#diagnosis
- https://www.babysfirsttest.org/newborn-screening/conditions/glucose-6-phosphate-dehydrogenase-deficiency
- https://www.egl-eurofins.com/tests/?testid=SAMPD
- https://www.mayoclinic.org/diseases-conditions/behcets-disease/symptoms-causes/syc-20351326
- Dr. Avinash's Blog
- Wikipedia
ACTIVE LEARNING AND CONVERSATIONAL DECISION SUPPORT TO TREATING TEAM OF THIS CASE :
[5/15, 23:41] Post Residency PG1: 👍
What is the efficacy of the various interventions she has been using and what is the sensitivity and specificity of the various diagnostic interventions she has undergone?
What other history, clinical findings and investigations would you need to solve her problem.
Also please check her latest update on her symptoms and another additional new diagnosis
[5/16, 14:38] MBBS 2016 UG 3: The latest update says that she is diagnosed with Behcet's disease
[5/16, 14:39] MBBS 2016 UG 3: So maybe Behcet's disease is the reason behind her rashes and mouth ulcers
[5/16, 14:41] MBBS 2016 UG 3: So...pathergy test may help us in confirming the doubt sir
[5/16, 20:10] Post Residency PG1: How was she diagnosed as Behchets disease?
[5/16, 23:34] MBBS 2016 UG 3: Maybe because she satisfied the criteria for diagnosis of Behcet's disese,i.e.,Recurrent mouth sores and skin lesions(major criteria) and genital ulcers
[5/16, 23:37] Post Residency PG1: Is it confirmatory? Ask the original poster if her pathergy test was positive
[5/17, 09:32] MBBS 2016 UG 3: Actually sir....There are no specific tests to confirm the diagnosis of behcet's....pathergy positive just gets us a bit choser to the suspicision...maybe only diagnostic criteria has to be looked into
[5/17, 10:23] Post Residency PG1: Good
So is their any weightage in the diagnostic criteria such as how many needs to be satisfied to increase the probability of the diagnosis?
[5/17, 21:00] MBBS 2016 UG 3: Yes sir...there is a fixed weightage for the diagnostic criteria to be satisfied.
It is as follows:
-->Presence of recurrent oral ulcerations for at least 3 times in an year
-->Plus any 2 of the following
-Recurrent genital ulcerations
-Eye lesions
-Skin lesions
-Positive pathergy test
[5/17, 21:06] Post Residency PG1: 👍
[5/17, 21:17] MBBS 2016 UG 3: Thank you sir

ReplyDeleteWhat is the efficacy of the various interventions she has been using and what is the sensitivity and specificity of the various diagnostic interventions she has undergone?
What other history, clinical findings and investigations would you need to solve her problem.
Also please check her latest update on her symptoms and another additional new diagnosis
[5/16, 2:38 PM] +91: The latest update says that she is diagnosed with Behcet's disease
ReplyDelete[5/16, 2:39 PM] +91: So maybe Behcet's disease is the reason behind her rashes and mouth ulcers
[5/16, 2:41 PM] +91: So...pathergy test may help us in confirming the doubt sir
[5/16, 8:10 PM] Rakesh Biswas: How was she diagnosed as Behchets disease?
[5/16, 11:34 PM] +91: Maybe because she satisfied the criteria for diagnosis of Behcet's disese,i.e.,Recurrent mouth sores and skin lesions(major criteria) and genital ulcers
[5/16, 11:37 PM] Rakesh Biswas: Is it confirmatory? Ask the original poster if her pathergy test was positive
[5/17, 9:32 AM] +91: Actually sir....There are no specific tests to confirm the diagnosis of behcet's....pathergy positive just gets us a bit choser to the suspicision...maybe only diagnostic criteria has to be looked into
[5/17, 10:23 AM] Rakesh Biswas: Good
So is their any weightage in the diagnostic criteria such as how many needs to be satisfied to increase the probability of the diagnosis?
[5/17, 9:00 PM] +91: Yes sir...there is a fixed weightage for the diagnostic criteria to be satisfied.
It is as follows:
-->Presence of recurrent oral ulcerations for at least 3 times in an year
-->Plus any 2 of the following
-Recurrent genital ulcerations
-Eye lesions
-Skin lesions
-Positive pathergy test