MITRAL STENOSIS
A 55 YEAR OLD WITH PALPITATIONS AND CHEST PAIN
FOLLOWING IS THE PROBLEM LIST ACCORDING TO PATIENT'S PRIORITY:
MAIN COMPLAINTS
Palpitations
Chest Pain
Shortness of breath
Bilateral Pedal Edema
Decreased Urine Output
EACH COMPLAINT IN DETAIL:
1.PALPITATIONS:
Since 2 months
Pounding character
POSSIBLE CAUSES:
- Cardiac causes:Mitral valve prolapse,pericarditis,congestive heart failure
- Non-cardiac causes:Hyperthyroidism, hypoglycemia
2.CHEST PAIN:
Since 2 months
On left side
More on epigastrium
Non-radiating type associated with the palpitations
POSSIBLE CAUSES:
-Myocardial infarction
-Mitral stenosis
-Acid reflux (ruled out as there is no dry cough or bitter taste)
-Pulmonary embolism
3.SHORTNESS OF BREATH:
Since 2 months
Progressive in nature
Present Status:Grade III-IV of dyspnea
Associated symptoms:
- Paroxysmal Noctural Dyspnea since 2 months--more since the last 10 days
- Wheeze on right side
- Coarse crepitations--more on right side than left side
POSSIBLE CAUSES:
- Respiratory cause(COPD,Pneumonia) -- ruled out as there are no symptoms such as cough,cold or wheeze
- Anemia
- Renal cause --ruled out as there is no facial edema
- Heart failure
4.BILATERAL PEDAL EDEMA:
Since 1 week
Upto Ankle
POSSIBLE CAUSES:
- Heart Failure
- Liver disease-- ruled out as there is no ascites
- Malnutrition --ruled out as there is no abdominal distention
- Thyroid disorder --rare
5.DECREASED URINE OUTPUT:
Since 1 week
Took medication for this outside
POSSIBLE CAUSES:
- Dehydration
- Kidney failure
- Heart failure--can lead to renal failure
PAST HISTORY:
- No similar complains in the past
- Not a known case of HTN,Diabetes,EPILEPSY,CVA,CAD
- No history of rheumatic fever
- No similar complaints in the family.
- No history of HTN, CAD, rheumatic heart disease, obesity, diabetes, sudden cardiac death.
- Mixed diet
- Appetite and Sleep-decreased
- Bowel&bladder-decreased urine
- Addictions-none
GENERAL EXAMINATION:
- He is conscious,coherent and cooperative,moderately built and nourished
- Afebrile
- Mild Dehydration
- Pallor absent
- No Icterus,cyanosis,clubbing,lymphadenopathy
- Edema upto ankles
- BP:110/70mmhg
- PR: feeble
ON EXAMINATION:
- dyspnoea-present (grade III-IV)
- wheeze-heard on right side
- trachea-central in position
- breath sounds- vesicular in nature, with coarse crepitations heard (right>left)
- Pulse- 72bpm, feeble, irregularly irregular, condition of vessel normal, pulse defecit could not be elicited.
- Normal except back-slight kypohosis present
- Mitral area:
-apex beat=changed, down and outward (in 6th intercostal space, in anterior axillary line)
-no thrills present
- Pulmonary area=normal
- Aortic area=normal
- Tricuspid area=loud S1 felt, no thrills
- No palpable pericardial rub,no tracheal tug.
- Cardiac rate=72bpm, irregularly irregular rhythm
- Mitral area=loud S1
- Tricuspid-loud S1
- Pulmonary area=splitting of S2-loud P2 component.
- No engorged veins
- Elevated jvp with larger "a" component
- Hepato-jugular reflex didnot elicit.
INVESTIGATIONS SHOWED:
LFT shows:
Elevated total and direct bilirubin
Elevated SGOT and ALP levels
- Elevated Urea
- Elevated Uric acid
- Elevated Calcium
- Elevated Phosphorus
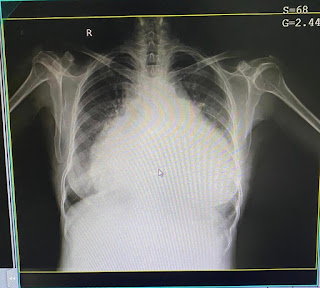
- Cardiomegaly
- Enlargement of right atrium, right ventricle, Left ventricle

- Irregular rhythm
- Absent p waves
- Right axis deviation
- ST elevation in V4 V5 aVR


Calcified mitral valves
Fish mouth appearance
ANATOMICAL LOCATION OF THE ROOT CAUSE:

Reference: https://www.grepmed.com/images/3141/palpitations-evaluation-cardiology-diagnosis-algorithm-ddxof
The pulse was feeble and irregularly irregular and ECG pattern suggest that palpitations are due to CARDIAC CAUSE
Shortness of breath(grade II-IV) is associated with paroxysmal nocturnal dyspnea, wheeze and coarse crepitations on right side which may be due to Pulmonary Edema
Source(https://medlineplus.gov/ency/article/000140.htm)says--
- As in this case,the edema is associated with shortness of breath and the ECG findings suggest of pathology related to HEART causing pulmonary hypertension-- The anatomical site of pathology most probably seems to be the HEART.
- Points not in favour of respiratory pathology are: No cough/hemoptysis/expectoration.
According tohttps://www.medscape.com/answers/163062-86210/what-causes-nocturia-and-oliguria-in-heart-failure --
- Oliguria indicates decreased blood supply to kidneys indicating CHRONIC HEART FAILURE.
- According to the symptoms and after the complete CVS examination, i am of the opinion that it could be a case of left heart failure.
- JVP is elevated with large 'a' component suggestive of Pulmonary Hypertension as a complication of left heart failure.
- 2D ECHO findings of calcified mitral valves and fish mouth appearance are suggestive of MITRAL STENOSIS.
PHYSIOLOGICAL FUNCTIONAL DISABILITY:
According to my knowledge:

Created by: Shivani
ETIOPATHOGENESIS:

Source: https://www.ijccm.org/book/9789352701926/chapter/ch57
DIAGNOSIS:MITRAL STENOSIS with HEART FAILURE
- INJ.LASIX 2amp in 50ml NS @8mg/hr --diuretic to treat edema
- oxygenation to maintain spO2 above 95%
- nebulization with budecort 12th hourly
- strict I/O charting
- monitoring BP,PR hourly
- inj.amiodarone 300mg (2amp) at 6ml/hr for irregular beats
- inj.pantop 40mg/OD/iv --to prevent gatric irritation
- T. ecosprin 75mg/PO/OD-- antiplatelet action to prevent clots
- fluid and salt restriction
- head end elevation
- Percutaneous balloon mitral valvuloplasty
- Mitral valve replacement
- Use of anticoagulants
- Beta blockers
- Davidsons principles of medicine

In this case, I don't think this is the question that begets maximum attention. Ideally once the problem representation is put out, a list of problems triaged according to those requiring maximum attention should be put forth. My 2 cents. She has quite a lot of problems that require immediate attention than her bilirubin levels. Also her peridcardial effusion seems to have been underestimated. A total of the size of effusion in anterior, posterior and lateral areas may well be above 2cm which makes it highly significant.
ReplyDeleteYes sir...bilirubin isn't as important as other problems which need more priority but i thought about it because bilirubin levels have inverse relation with risk of cardiovascular disease..according to some sources...so had that doubt about bilitubin sir
DeleteSir...did the patient have pericardial effusion...
ReplyDeletethen what was the colour of the fluid on pericardial tap sir??