HEART FAILURE
A 35 YEAR OLD WITH SHORTNESS OF BREATH AND PEDAL EDEMA
I've been given this case data to solve in an attempt to understand and analyize the topic based on patient clinical data in order to develop competency in reading and comprehending clinical data related to the case and come up with a suitable diagnosis.
You can find the original case in the link below-
https://madhur116.blogspot.com/2020/05/on-1452020.html
https://hitesh116.blogspot.com/2020/05/elog-14th-may-2020.html
FOLLOWING IS THE PROBLEM LIST ACCORDING TO PATIENT'S PRIORITY:
MAIN COMPLAINTS(Chronologically):
- FEVER
- SHORTNESS OF BREATH
- BILATERAL PEDAL EDEMA
- GENERALISED WEAKNESS
EACH COMPLAINT IN DETAIL:
1.FEVER
- 1 month back
- High grade fever
- Associated symptoms:Chills
- PROBABLE CAUSES:
- Viral infection
- Malaria
- Meningitis (on examination, CNS is found to be normal--thus ruled out)
- Typhoid fever( ruled out as there is no abdominal pain or rashes associated with fever)
- Treatment:
- was treated symptomatically
- was given Antimalarials
2.SHORTNESS OF BREATH
- Since 2 weeks
- Initially was NHYA Grade 3
- Regressed to Grade 2 after treatment
- Associated symptoms: Paroxysmal Nocturnal Dyspnea
- PROBABLE DIAGNOSIS
- Respiratory cause(COPD,Pneumonia) -- ruled out as there are no symptoms such as cough,cold or wheeze
- Anemia
- Renal cause --ruled out as there is no associated oliguria or facial edema
- Heart failure
- Pitting type
- Progressive in nature
- Extent: Upto knees
- PROBABLE DIAGNOSIS:
- Heart Failure
- Liver disease (ascites is present but it is mild-not as prominent as pedal edema -- thus may not be related to liver)
- Malnutrition --ruled out as there is no abdominal distention
- Thyroid disorder --rare

4.GENERALISED WEAKNESS:
- DURATION: from 2 weeks
- PROBABLE CAUSES:
- Asthma -- ruled out as there is no wheeze or cough
- Heart failure
- Shock
PAST HISTORY:
- No similar complains in the past and no H/O Trauma
- Not a known case of HTN,Diabetes,EPILEPSY,CVA,CAD
PERSONAL HISTORY:
- Mixed diet
- Appetite and bowel and bladder habits are normal
- H/O Alcohol and smoking occasionally
GENERAL EXAMINATION:
- He is consious,coherent and cooperative,well built and well nourished
- Afebrile
- Pallor absent
- No Icterus,cyanosis,clubbing,lymphadenopathy
- Edema upto knees (grade2)
- BP:130/80mmhg
- PR:80bpm
ON EXAMINATION:
- CVS: S1, S2heard
- RS: right ISA early inspiratory crepts +
- P/A:soft and non tender
- CNS:
- High mental functions normal
- Cranial nerves intact
- Motor and Sensory system normal
- No meningeal and cerebellar signs
ON EXAMINATION OF NECK:
- JVP: was found to be raised(20 cm of H2O)
- visible in 45 degrees near clavicle and at 90 degrees
INVESTIGATIONS SHOWED:
All were normal except:
Post Prandial Blood Sugar levels were HIGH
HDL was low
ECG:

USG Abdomen
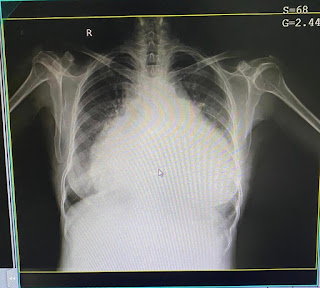
- Right moderate pleural effusion
- Grade 1 fatty liver and mild ascites

2D ECHO shows:
REFERENCE:
- EF-27%
- IVC dilated(2.3cm)not collapsing
- end point septal separation distance is increased
- mild TR+,severe MR+,trivial AR+
- dilated all chambers
- global hypokinesia
- severe LV dysfunction
- mild PAHT
- no MS/AS,no PE/LV clot
According to this reference link-http://www.meddean.luc.edu/lumen/MedEd/MEDICINE/medclerk/2004_05/level1/Lungs/lungs_f.htm
- The information goes as follows:
"Typically, early inspiratory crackles are associated with congestive heart failure while pan-inspiratory or late inspiratory crackles are associated with diffuse interstitial pulmonary fibrosis."
- In this case,on auscultation,early inspiratory crepts are heard in the right interscapular area
- So,the problem is with the HEART
According to the following reference resource-
- "In normal individuals this has little effect on lungs, but in patients in whom the additional volume cannot be pumped out by the left ventricle due to left ventricular weakness, there is a significant reduction in lung capacity which results in shortness of breath. Additionally, in patients with congestive heart failure the pulmonary circulation may already be overloaded because of the failing left ventricle. When a person lies down, the left ventricle is unable to match the output of a more normally functioning right ventricle on increased venous return to the lungs; causing pulmonary congestion thus leading to Paroxysmal Noctural Dyspnea(Shortness of breath during sleep)."
Bilateral Pitting type of pedal Edema can occur due to congestive Heart failure or kidney disease or cirrhosis of liver--to find the organ responsible.....
- Following source says--https://www.aafp.org/afp/2013/0715/p102.html
"Echocardiography to evaluate pulmonary arterial pressures is recommended for patients with obstructive sleep apnea and edema. In one study of patients with obstructive sleep apnea, 93% of those with edema had elevated right arterial pressures.Pulmonary hypertension has long been thought to be the cause of edema associated with obstructive sleep apnea. However, one study found that although a high proportion of patients with edema had obstructive sleep apnea (more than two-thirds), nearly one-third of these patients did not have pulmonary hypertension, which suggests a stronger correlation between edema and obstructive sleep apnea than can be explained by the presence of pulmonary hypertension alone."

- As in this case,the edema is associated with shortness of breath and the ECG findings suggest of pathology related to HEART causing pulmonary hypertension-- The anatomical site of pathology most probably seems to be the HEART.
Increased sympathetic nerve activity, which involves the nerves that carry adrenaline, also occurs in people with heart failure. It is possible that the increased sympathetic nerve activity may actually cause the leg muscle weakness.
--Reference:https://clinicaltrials.gov/ct2/show/NCT00858845
PHYSIOLOGICAL FUNCTIONAL DISABILITY:

Reference:

ETIOPATHOGENESIS:
- Symptoms for left heart failure are DSYPNEA and WEAKNESS
- Symptoms of right heart failure are ASCITES and PEDAL EDEMA
- Our patient has all these symptoms,so maybe he has CONGESTIVE HEART FAILURE
- Left-sided CHF is the most common type of CHF. It occurs when your left ventricle doesn’t properly pump blood out to your body. As the condition progresses, fluid can build up in your lungs, which makes breathing difficult.
- Right-sided CHF occurs when the right ventricle has difficulty pumping blood to your lungs. Blood backs up in your blood vessels, which causes fluid retention in your lower extremities, abdomen, and other vital organs.
- It’s possible to have left-sided and right-sided CHF at the same time. Usually, the disease starts in the left side and then travels to the right when left untreated.
- According to the source--https://pubmed.ncbi.nlm.nih.gov/7713107/
- In this case, the EF is less then 40 percent.
- Thus, this is a case of SYSTOLIC FAILURE /HEART FAILURE DUE TO REDUCED EJECTION FRACTION.
- Since there is a history of fever with chills, the most likely cause for this type of heart failure according to my opinion may be VIRAL INFECTION ==> VIRAL MYOCARDITIS
- According to the 2D ECHO findings, all chambers are dilated ==> indicates DILATED CARDIOMYOPATHY.
DIAGNOSIS:
Heart failure with reduced ejection fraction secondary to viral myocarditis with denovo DM type 2
TREATMENT:
- PHARMACOLOGICAL:
- Tab.lasix 80mg...40mg...40mg --Diuretic to treat edema
- Tab.isosorbide mononitrate10mg bd
- Tab.hydralazine 25mg --for Hypertension and heart failure
- Tab. Telma20mg --for hypertension and heart failure
- Tab.metformin 500mg po od -- for treating Diabetes type 2
- NON-PHARMACOLOGICAL:
- Fluid restriction <1litre/day
- Salt restriction <2gms/day
TREATMENT SUGGESTED:
- Angiotensin converting enzyme (ACE) inhibitors
- Angiotensin receptor-neprilysin (ARN) inhibitors
- Angiotensin receptor blockers (ARBs)
- Beta-blockers (BBs)
RECENT ADVANCES:
Based on the above findings, the dosage of vymarda 50mg BD(sacubitril 26mg +valsartan24mg)has been increased to vymarda to 100 mg BD
- Davidsons principles of medicine
ACTIVE LEARNING AND CONVERSATIONAL DECISION SUPPORT TO TREATING TEAM OF THIS CASE :
[5/28, 23:35] MBBS 2016 UG 3: Sir...in the 35 yr old case...on examination of respiratory system:the case says right ISA early inspiratory crepts
Sir...what does ISA mean?
[5/28, 23:39] MBBS 2016 UG 3: Is it interscapular area sir?
[5/29, 11:16] Post Residency PG1: Yes but please do ask all these to the treating unit people also
[5/29, 11:23] MBBS 2016 UG 3: Ok sir

This comment has been removed by the author.
ReplyDeleteWhy all these were suggested? They cannot be taken altogether.
ReplyDeleteAngiotensin converting enzyme (ACE) inhibitors
Angiotensin receptor-neprilysin (ARN) inhibitors
Angiotensin receptor blockers (ARBs)
Sir...The best suitable medication from those are to be given....not all together
DeleteAnd sir...according to my knowledge...maybe ACE inhibitors are the best because they help in relaxing the blood vessels and help blood flow easily