Case wise Active learning and discussion-5
Case 5-- Heart Failure
A 35 YEAR OLD WITH SHORTNESS OF BREATH AND PEDAL EDEMA
We the MBBS final year students have been given these cases on weekly basis to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
- Link to Reference:
- Link to my analysis:
ACTIVE LEARNING AND CONVERSATIONAL DECISION SUPPORT TO TREATING TEAM OF THIS CASE :
- My active learning discussion:
[5/28, 23:35] MBBS 2016 UG 3: Sir...in the 35 yr old case...on examination of respiratory system:the case says right ISA early inspiratory crepts
Sir...what does ISA mean?
[5/28, 23:39] MBBS 2016 UG 3: Is it interscapular area sir?
[5/29, 11:16] Post Residency PG1: Yes but please do ask all these to the treating unit people also
[5/29, 11:23] MBBS 2016 UG 3: Ok sir
- OTHER DISCUSSIONS:
[5/30, 16:22] MBBS 2016 UG Student 20: http://meghana140.blogspot.com/2020/05/heart-failure-in-35-year-old-male.html
Few doubts i got while writing the case:
1.Is the mitral regurgitation in this case secondary to left ventricular dysfunction or is it the regurgitant valvular disease that is causing the heart failure?
2.What are the long term complications of using diuretics?
[5/30, 16:32] MBBS 2016 UG student 25: Mitral regurgitation in this case is due to left ventricular dilatation (which is due viral myocarditis) which stretches the mitral valve anulus causing valvular insufficiency
[5/30, 16:33] MBBS 2016 UG student 25: https://www.cardiomyopathy.org/news--media/latest-news/post/420-mitral-valve-regurgitation
[5/30, 16:39] MBBS 2016 UG Student 20: 👍
[5/30, 16:46] MBBS 2016 UG student 26: Regarding your question 2.
“The most worrisome effects of diuretic therapy have revolved around hypokalemia and its relationship to cardiac arrhythmias and sudden death.”
https://www.ahajournals.org/doi/pdf/10.1161/01.HYP.11.3_Pt_2.II16
[5/30, 17:03] Post Residency PG1: Please share scientific links to any statement you make. Particularly the comment "overload on left ventricle"
[5/30, 17:05] MBBS 2016 UG Student 22: https://www.mdmag.com/journals/cardiology-review-online/2007/may2007/may-2007-mallis-commentary
[5/30, 17:06] Post Residency PG1: Please quote from the relevant portions that you want us to focus on
[5/30, 17:07] Post Residency PG1: What is the evidence that she has mitral regurgitation?
[5/30, 17:07] Post Residency PG1: Ask the treating team to share her Echo video
[5/30, 17:08] Post Residency PG1: Oh it's the 35M. I thought it was the 55F
[5/30, 17:10] MBBS 2016 UG Student 22: Ok sir
[5/30, 17:19] MBBS 2016 UG Student 3: Elevation of left atrial pressures leads to pulmonary venous hypertension, which leads to reduced compliance of the lungs and a decrease in vital capacity, resulting in Dyspnea.
Dyspnea on exertion may be related to an inability to increase the cardiac output due to impaired left ventricular filling leading to a low end diastolic volume.
[5/30, 17:21] Post Residency PG1: 👍Yes but what is the mechanism of that feeling of dyspnoea which is defined as an abnormal awareness of one's own normal breathing
[5/30, 18:08] MBBS 2016 UG Student 3: "It is thought that three main components contribute to dyspnea: afferent signals, efferent signals, and central information processing. It is believed the central processing in the brain compares the afferent and efferent signals; and dyspnea results when a "mismatch" occurs between the two: such as when the need for ventilation (afferent signaling) is not being met by physical breathing (efferent signaling)."
Reference:
Harrison's Principles of Internal Medicine (Kasper DL, Fauci AS, Longo DL, et al. (eds)) (16th ed.). New York: McGraw-Hill.
[5/30, 18:10] MBBS 2016 UG Student 3: Does Pulmonary venous hypertension lead to Pulmonary interstitial edema?
[5/30, 18:12] MBBS 2016 UG Student 3: If yes,
The development of interstitial edema could lead to the stimulation of C-fibers.
C-fibers are unmyelinated afferent nerve fibers that originate in J-receptors located in small airways and near alveolar capillaries; they are stimulated by mechanical and chemical factors. The stimulation of the J-receptors causes a reflex increase in breathing rate, and is also thought to be involved in the sensation of dyspnea.
[5/30, 18:22] MBBS 2016 UG Student 2: https://rhea9895.blogspot.com/2020/05/case-of-35-years-old-male-with-i-have.html
[5/30, 18:23] MBBS 2016 UG Student 2: Things which I did not understand in this case are:
1)Why was Anti-malarial drug prescribed for him if it was a simple viral fever? Why not Paracetamol/ Ibuprofen?
2)What were his auscultatory findings?
[5/30, 20:16] Post Residency PG1: 👍 So would the J receptors and C fibers be stimulated also by airway resistance as that also causes dyspnoea? Let's look at scientific studies and not just text book assumptions.
[5/30, 20:19] Post Residency PG1: 👍
1) unfortunately people are prescribing it for the big virus troubling mankind the most now
2) We have the patient's number if any of you can help us take a better history. Also the auscultation point is giving me an idea. Can we collect the patient's heart sounds also through his mobile phone by asking him to place it in different locations of his chest?
[5/30, 20:24] MBBS 2016 UG Student 2: Sir there are studies which say that Chloroquine can cause cardiomyopathy. So could that be possible in this case? Assuming he was prescribed chloroquine.
[5/30, 20:25] MBBS 2016 UG Student 13: He was prescribed Choloquine according to a PG Maam.
[5/30, 20:26] MBBS 2016 UG Student 2: Okay. So could that be the cause?
https://www.tandfonline.com/doi/abs/10.3109/08923973.2013.780078?src=recsys&journalCode=iipi20&
[5/30, 22:05] Post Residency PG1: Is this a quote from the link below? 🤔
[5/30, 22:52] Post Residency PG1: Does our case fit with the case described here?
[5/30, 22:59] MBBS 2016 UG Student 3: Effects of bronchoconstriction and external resistive loading on the sensation of dyspnea:
https://journals.physiology.org/doi/abs/10.1152/jappl.1991.71.6.2183
This study compared the sensation of difficulty in breathing during isocapnic voluntary hyperventilation in six normal subjects.
"To clarify the role of vagal afferents on the genesis of dyspnea during both forms of obstruction to airflow, the effect of airway anesthesia by lidocaine aerosol inhalation was also examined after histamine and during external resistive loading."
"Histamine inhalation significantly increased the intensity of the dyspneic sensation over the equivalent external resistive load at the same levels of ventilation and occlusion pressure during voluntary hyperpnea. Inhaled lidocaine decreased the sensation of dyspnea during bronchoconstriction with no change in Raw, but it did not significantly change the sensation during external resistive loading. These results suggest that afferent vagal activity plays a role in the genesis of dyspnea during bronchoconstriction."
[5/30, 23:01] Post Residency PG1: And where do the vagal afferents relay to convey this sensation of dyspnoea? Also are they connected to the J receptors in the alveoli or some other receptors?
[5/30, 23:02] MBBS 2016 UG Student 2: No sir it mainly shows the long term effects of chloroquine
[5/30, 23:04] Post Residency PG1: Will be looking forward to your finding a chloroquin study that demonstrates acute cardiac damage similar to what our patient had. Any takers for direct history taking in this patient through telephone including his mobile phone auscultation data?
[5/30, 23:09] MBBS 2016 UG Student 3: Afferent information from reflex stimulation of the peripheral sensors (chemoreceptors and/or vagal C fibers) is processed/relayed centrally in the limbic system, especially the insular area and sensorimotor cortex.
A perturbation in the ventilatory response due to weakness, paralysis, or increased mechanical load generates afferent information from vagal receptors in the lungs (and possibly mechanoreceptors in the respiratory muscles) to the sensorimotor cortex and results in the sensation of dyspnea.
[5/31, 08:18] MBBS 2016 UG Student 13: https://caseopinionsbyrollno156.blogspot.com/2020/05/fighting-for-breath.html
Some doubts:
1.What was the dosage of Chlorquine given to him? What was the treatment he recieved for improvement from Grade 3 NYHA to grade 2?
2. Why is there presence of early inspiratory crepts in this patient with pleural effusion, when early inspirtaoy crepts indicate Chronic Obstructive Pulmonary Disorders?
3. Why did pleural effusion occur and not pulmonary edema when mechanism of rise of backflow pressures from left atrium is the same in both?
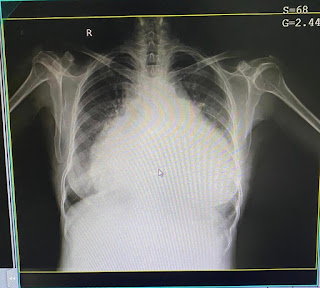
4. Why was no chest X-ray taken to better understand the lung pathology?
5. How was a severe Mitral reguritation hidden? There was no systloic murmur neither any characteristic ECG changes?

Comments
Post a Comment